The Tri-Cycle Hypothesis – A New Theory of Type 2 Diabetes (sort of)
Dr. Sean Wheatley, MSc, PhD; Science and Research Lead at X-PERT Health.
Sean.Wheatley@xperthealth.org.uk
Few ideas have done more to change how we understand type 2 diabetes than Professor Roy Taylor’s twin cycle hypothesis. But what if the name misses something out?
Understanding the causes of a disease is important if we are going to understand how best to treat it, and type 2 diabetes is no exception. Although not all people with type 2 diabetes experience raised blood glucose levels for the same reasons, the twin cycle hypothesis appears to explain what is happening for a high proportion of them. In this month’s blog we take a look at this theory, and why there might be a bit missing (from the name at least).
Cycle 1 – The Liver
As the name implies, the twin cycle hypothesis describes two cycles within the body which, over time, can lead to type 2 diabetes.
The first of these occurs in the liver. Indeed, Professor Taylor has previously described “the long, silent scream of the liver” that can often be detected before an individual experiences type 2 diabetes. This underlines its importance.
In simple terms, this cycle occurs when there is an increase in fat within the liver which reduces its ability to perform all its functions properly.
One of the liver’s functions is to release a slow and steady stream of glucose into the blood when we have not eaten, to prevent blood glucose levels dropping too low; and to stop doing this when we have eaten something that contains carbohydrate, to help prevent it going too high. This latter part is triggered by insulin – when we eat something containing carbohydrate, insulin levels are increased, and this tells the liver to stop releasing glucose. Essentially, the insulin turns off the tap.
But when fat storage in the liver reaches a certain level, it reduces the liver’s ability to respond to insulin. This is known as “insulin resistance”. When there is insulin resistance in the liver, the glucose tap does not get switched off when it should. The liver therefore keeps releasing glucose into the blood, even though glucose is also entering the blood from the food that has been eaten. Blood glucose levels increase as a result.
This can become a vicious cycle, as insulin resistance and the increase in blood glucose levels both lead to the release of extra insulin, which leads to an increase in fat storage (including in the liver), continuing the cycle.
Cycle 2 – The Pancreas
The second cycle happens in the pancreas. Much like the liver cycle, the simple version is that an increase in fat storage in the pancreas impairs its function. In this case, it affects the specialist cells which produce and release insulin.
In relation to the development of type 2 diabetes, the most important impact is the loss of the first-phase insulin response. This is when the pancreas quickly releases some insulin after we have eaten something containing carbohydrate, with the main purpose being to shut down the release of glucose from the liver (as described in the previous section).
Without the first-phase insulin response the liver does not receive the signal to stop releasing glucose into the blood. Blood glucose levels therefore rise higher than they should do, as glucose is entering from both the liver and from the food (again, as noted before). This makes the pancreas have to work even harder, which can lead to further reductions in its ability to function properly. The high glucose levels can also have a direct negative impact on the pancreas too – this is called “glucotoxicity”. These factors, combined with further fat storage when insulin levels are increased, continue the cycle within the pancreas.
The Twin Cycle Hypothesis
The key driver of each of these cycles is therefore the build-up of excess fat within them. This has important implications for how type 2 diabetes can be prevented, managed, treated, or potentially even reversed, as we will touch upon later.
It is also worth noting though that these two cycles do not occur separately from each other – hence we end up with a “twin cycle” rather than two independent ones. That is to say, the negative effects occurring in either of these organs can, and do, have an impact on the other. For example:
– An increase in liver fat results in the liver releasing extra fat into the blood. Some of this ends up in the pancreas, causing or increasing the storage of fat there, and (further) impairing the function of the pancreas.
– The increase in blood glucose levels caused by the impaired function of the pancreas ultimately leads to an increase in total insulin levels. This can lead to an increase in fat storage in the liver, which (further) impairs liver function.
There is therefore a cycle occurring within the liver, a cycle occurring within the pancreas, and a cycle occurring between the liver and pancreas. Without any steps being taken to address at least one of these cycles, things will continue to get worse. Eventually, the body’s ability to maintain blood glucose within a “normal” range runs out, leading to prediabetes and then type 2 diabetes.
Cycle 3 – The Muscles
This is where “my” theory, or at least my thoughts on how the twin cycle hypothesis might underemphasise something, come in.
Essentially, there is arguably a third significant cycle occurring in the skeletal muscles* that is worth including. It is worth noting that muscle is alluded to in the diagram used to outline the twin cycle hypothesis (see Figure 6 in this article, for example). Its inclusion in the “tri-cycle hypothesis” is not therefore really new, and so nor is the tri-cycle hypothesis itself (and I am not trying to suggest it is). The reference to the muscles in the twin cycle hypothesis is by a single arm leading into the liver cycle though, which notes “pre-existing muscle insulin resistance” (alongside “positive calorie balance”) as a driver of increased liver fat. It is not therefore given a great deal of focus.
However, skeletal muscle has a significant influence on metabolic health, including in relation to blood glucose control and weight management. This includes as a major destination for glucose (and fat), for energy usage and storage. The skeletal muscles also have a major impact on weight management through their impact on basal metabolic rate (BMR) – the more skeletal muscle we have, the higher our BMR, the easier it is to manage body weight.
When it comes to skeletal muscle being considered as a potential third cycle which is worthy of being included in the theory of type 2 diabetes development, the steps which would be most comparable to those outlined for the liver and the pancreas before would be that:
– An increase in fat storage in the skeletal muscle and/or an increase in blood glucose levels can cause an increase in skeletal muscle insulin resistance.
– Impaired functionality in the skeletal muscle (because of the insulin resistance) then leads to an increase in blood glucose levels (because of reduced uptake of glucose by the skeletal muscles).
– The increase in blood glucose levels leads to an increase in insulin levels, which causes a further increase in fat storage and insulin resistance in the skeletal muscle (thus restarting the cycle).
The Tri-cycle Hypothesis
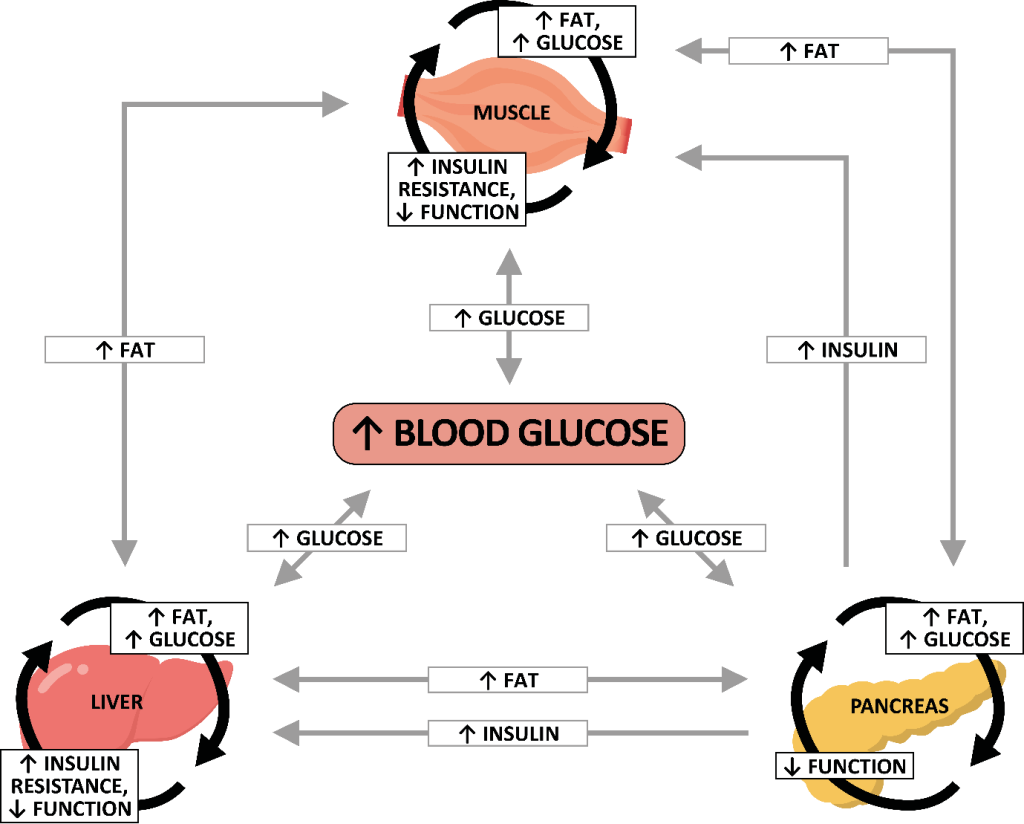
Adding this to the twin cycle hypothesis is then relatively straightforward, with the links being consistent with those we have already discussed between the liver and pancreas. This is outlined in the diagram below, but in a nutshell:
– All three cycles (i.e., in the skeletal muscle, liver and pancreas) can directly increase blood glucose levels. This can then impact the other cycles.
– All three cycles can result in the increased release of fat into the blood, as each of the relevant organs can push some fat out when more is being stored within them than they would like**. This can then impact the other cycles.
– The additional insulin being released by the pancreas can increase insulin resistance and fat storage in both the liver and skeletal muscle, causing further impairments in their functionality.
So, as well as vicious cycles occurring within each of these parts of the body, there are also vicious cycles occurring between all of them. As with the twin cycle hypothesis, without appropriate action being taken the body’s ability to manage blood glucose levels will likely get worse and worse over time.
Implications for Treatment
It is beyond the scope of this blog to explore treatments in detail, but any shift in thinking about the cause of type 2 diabetes would only really matter to people living with this condition if it affected how it was treated. We will therefore take a quick look at this before wrapping things up.
The main treatment-based conclusion from the twin cycle hypothesis is the importance of fat loss. Most importantly, if you can reduce the amount of fat that is stored in the liver and pancreas you can improve how well they work. This can then lead to improvements in blood glucose control, and potentially the remission of type 2 diabetes. The results of multiple studies, most notably DiRECT (a clinical trial led by Professor Taylor, alongside Professor Mike Lean), back this up.
Carbohydrate restriction is another viable avenue for improving diabetes management, in line with the core premises of the twin cycle hypothesis. This is because it will reduce post-meal glucose levels and the amount of insulin that is needed, with positive effects on the cycles within both the liver and pancreas. Again, research supports the potential benefits of low carbohydrate approaches for the management and potential remission of type 2 diabetes.
As the tri-cycle hypothesis still contains all the elements of the twin cycle hypothesis, fat loss would also be considered the primary avenue for treatment, with carbohydrate restriction still an option too. Both of these interventions are still relevant as options for trying to improve skeletal muscle function (and so for interfering with the skeletal muscle cycle) as well.
What the inclusion of this third cycle would perhaps do though, is add an additional focus on building and maintaining muscle mass. The value of skeletal muscle in managing blood glucose is well known, with skeletal muscle providing one of the most important “sinks” for absorbing additional glucose. More skeletal muscle (and/or better functioning skeletal muscle) essentially means there is a greater capacity for removing the glucose from the blood. An increased focus on this, for example through the promotion of resistance exercise (e.g., taking part in exercise that makes the muscles work against a resistance at least a couple of times each week) and sufficient protein intake (e.g., building meals around one or two portions of protein), may therefore help to improve the management of type 2 diabetes.
So, What’s the Bottom Line?
The twin cycle hypothesis is (probably) the most widely accepted explanation of type 2 diabetes. It focuses on how the build-up of fat in the liver and pancreas affects how well these organs work, and how this creates multiple vicious cycles which can eventually cause type 2 diabetes. There is perhaps an argument though that there is a third cycle which isn’t adequately reflected in this theory, involving the skeletal muscles. Skeletal muscle has an important impact on blood glucose management, and weight management more broadly. Increasing focus on this, and encouraging the building and maintenance of muscle mass alongside a focus on weight loss when trying to prevent or manage type 2 diabetes, may therefore have benefits.
The twin cycle hypothesis transformed how we think about type 2 diabetes — perhaps it’s time to add a third wheel.
* The skeletal muscles are the muscles that attach to our skeleton to allow us to move – when they contract, they pull the bones, which creates the movement. They are ultimately therefore the muscles people tend to think of when you say “muscle” anyway, but I thought it was worth clarifying.
** It is worth noting that the degree to which this occurs will usually be much less from the skeletal muscle than the liver or pancreas, though excess fat within the muscle can still contribute to a general flux of fat throughout the body to some degree.
